 Intelligent Design
Intelligent Design
 Medicine
Medicine
Nathan Lents Is Back; Still Wrong About Sinuses

As long experience teaches, critics of intelligent design tend to divide neatly into two categories. There are those who primarily want to attack motives, make false accusations of deception and dishonesty, and engage in creative name-calling. On the other hand, there are serious and thoughtful critics. Sometimes the latter are misled about ID by the former.
This distinction may help explain what happened recently when biologist and ID-critic Nathan Lents was given an open forum to sound off on Discovery Institute. This occurred at the website Peaceful Science, hosted by another critic of ID, biologist and MD Joshua Swamidass. The interaction with Lents is of interest because it provides an opportunity to look again, in some detail, at a fascinating illustration of design in action.
A Nose for Bad Arguments
Earlier this year writers for Evolution News posted responses to Dr. Lents, who teaches at John Jay College and wrote a recent book, Human Errors: A Panorama of Our Glitches, from Pointless Bones to Broken Genes. He argues that our bodies demonstrate “poor design” or “suboptimal design” which is best explained by evolution. Lents wrote an opinion piece for the Wall Street Journal summarizing his case.
He argues in his book that the fact that the openings to the maxillary sinuses (called “ostia”) are situated near the top of the sinuses would prevent gravity drainage of mucus. This, he thinks, is bad design. He asks, “What kind of plumber would put a drainpipe anywhere but at the bottom of a chamber?” Neurosurgeon Michael Egnor, who knows a thing or two about the anatomy of the head, replied to Lents, here and here. Egnor explained that the design of the maxillary sinuses makes sense for several reasons, as follows.
Though excess mucus is annoying when you catch a cold, mucus is a normal and necessary bodily fluid that is secreted by mucus membranes. Its multiple important purposes include preventing tissues from drying out, trapping harmful foreign bodies such as bacteria or allergens, and serving as a locality for antibodies and other enzymes that are “designed to kill or neutralize these harmful materials.” Egnor points out that if the maxillary sinus drained from the bottom, it might quickly lose its vital mucus. This would cause problems: “From design considerations, it can be inferred that a drainage ostium in the floor of the sinus would drain at too high a rate, drying out the sinus mucosa and predisposing to plugging of the ostium by thick debris.”
Cilia move mucus upwards, against the flow of gravity, towards the ostia in the maxillary sinus. In fact, as Egnor observes, our paranasal sinuses “don’t drain primarily by ‘gravity,’ as Lents naïvely asserts,” meaning that the fact that the opening in the maxillary sinus is at the top is immaterial to how it normally drains.
Another observation Egnor made is that even from a gravity-drainage perspective, there could be rational reasons for putting the drainage opening at the top of the sinus. Plumbers frequently put drains at the tops of chambers. A possible purpose for situating the ostia at the top of the maxillary sinuses is so they can serve as “overflow openings,” much like the drains located at the tops of sinks or bathtubs.
Lastly, Egnor observed that the maxillary sinuses can have other methods of drainage that don’t depend on gravity, called “accessory ostia,” located further down towards the bottoms of the sinus.
A Relevant Paper
On that last point, Egnor cited a paper, “The Drainage System of the Paranasal Sinuses: A Review with Possible Implications for Balloon Catheter Dilation,” which he quoted. The paper states, “Accessory ostia are not only common for the maxillary sinus but also for the entire paranasal sinus system.” After reviewing the design of the paranasal sinuses, Egnor concluded:
For most of humanity’s seven billion people, paranasal sinuses drain flawlessly for the better part of a century without any tinkering at all. “Poor” design? If sinks and toilets drained as well as sinuses, plumbers would be mostly out of work.
On his own blog, Lents replied to Egnor by arguing that the paper Egnor cited is about the paranasal sinuses, not the maxillary sinus:
First of all, if you carefully read both what he wrote, and especially the paragraph that he provides as his source, you will notice that most of it is discussing accessory drainage in the paranasal and frontal sinuses, not the maxillary sinuses. The paranasal and frontal sinuses surround your nose and are in your forehead, respectively. Nothing I write in my book or articles make reference to those sinuses. My “poor design” argument is about the maxillary sinuses only.
Now, at Joshua Swamidass’s discussion forum, Lents claims again that Egnor was wrong to cite this “completely off-topic paper” because it isn’t about the maxillary sinuses:
You will notice that the article is all about the paranasal sinuses not the maxillary sinuses. Totally different structures!
Lents uses Swamidass’s forum to rant at us, saying that we’re “dishonest” and claiming Dr. Egnor was just trying to take advantage of ignorant readers. In Lents’s words, “They made an obvious error, got caught, and then just pretend it didn’t happen.”
No, there was no error to correct. On the contrary, it’s Lents’s description of nasal anatomy that is wrong, at an elementary level. The maxillary sinus and the paranasal sinuses are not “totally different structures.” The maxillary sinus is one of the paranasal sinuses! The paper Egnor cited was discussing the maxillary sinus as well as the other paranasal sinuses.
Lents similarly writes on his blog, “The paranasal and frontal sinuses surround your nose and are in your forehead, respectively. Nothing I write in my book or articles make reference to those sinuses.” Again, that’s not true because, to repeat, the maxillary sinus, which Lents indeed writes about in his book, is one of the paranasal sinuses, meaning that Lents does write about the paranasal sinuses. He is wrong in his terminology.
What the Article Says
Interestingly, Lents doesn’t quote from the article itself. Here’s some of what it says:
- “Intersinus connections and accessory ostia of the maxillary sinus are well known to rhinologic surgeons but are less known for the remaining paranasal sinuses.”
- “Accessory ostia are not only common for the maxillary sinus but also for the entire paranasal sinus system.”
- “Expansion of the mucous membranes helps to form the paranasal sinuses: the maxillary sinus, the ethmoid cells, and the frontal and sphenoid sinuses, respectively.”
Some of that is technical language. What’s clear is that the paper that Egnor cited frequently discusses the maxillary sinus, and the maxillary sinus is one of the four paranasal sinuses. When it states that “Accessory ostia are not only common for the maxillary sinus but also for the entire paranasal sinus system,” it is not, as Lents says, “completely off-topic” but rather directly on-topic. It is indicating that accessory ostia are “common for the maxillary sinus.”
Paranasal sinuses are a group of four paired air-filled spaces that surround the nasal cavity. The maxillary sinuses are located under the eyes; the frontal sinuses are above the eyes; the ethmoidal sinuses are between the eyes and the sphenoidal sinuses are behind the eyes. The sinuses are named for the facial bones in which they are located.
[…]
Humans possess four paired paranasal sinuses, divided into subgroups that are named according to the bones within which the sinuses lie:
The maxillary sinuses, the largest of the paranasal sinuses, are under the eyes, in the maxillary bones (open in the back of the semilunar hiatus of the nose). They are innervated by the trigeminal nerve.
A picture on Wikipedia’s “Paranasal sinuses” page shows the four different paranasal sinus cavities — one of which is the maxillary sinus:
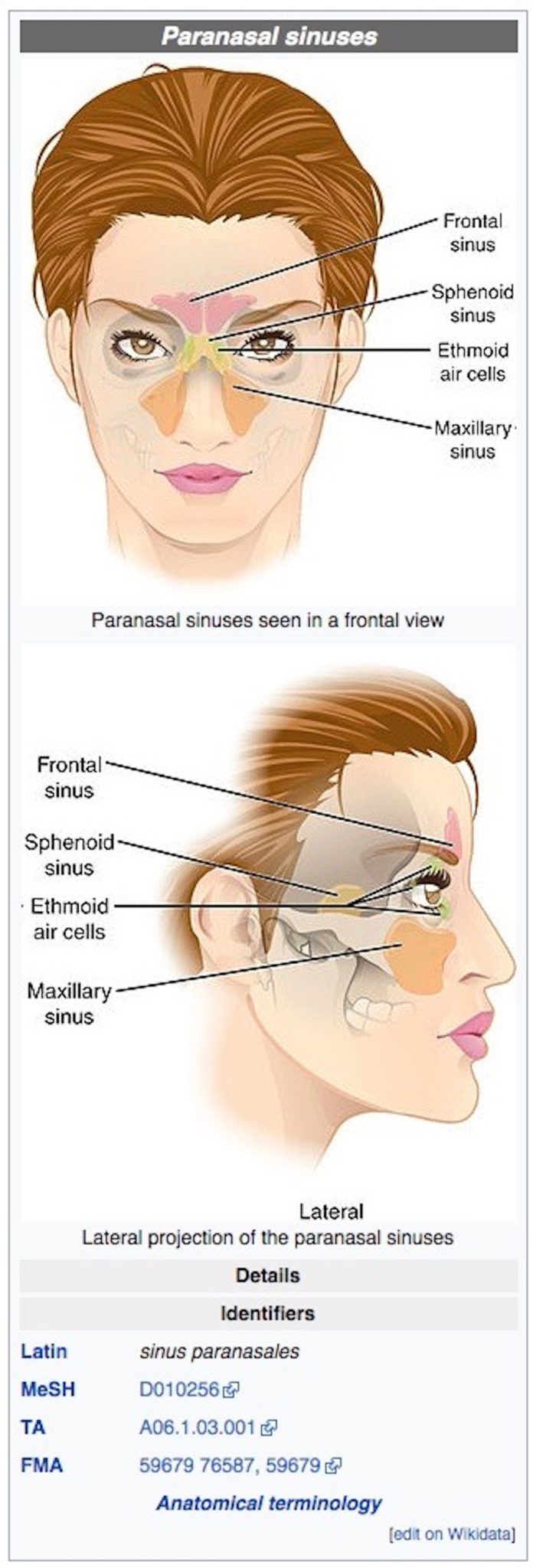
Image credit: OpenStax College [CC BY-SA 3.0 ], via Wikimedia Commons.
{kind=link}
This is basic physiology, and Lents gets it wrong when he claims that the maxillary sinus is not a paranasal sinus.
In his blog reply Lents goes on to argue that the accessory ostia in the maxillary sinus don’t resolve the issue since not all people have them. (Lents claims only up to 30 percent do although the literature states they exist in up to 43 percent of people.) These accessory ostia are not fully understood, and researchers have debated the matter. Studies have asked whether they are congenital (i.e., present naturally at birth) or whether they arise during a person’s lifetime due to sinusitis or other pathologies. One paper notes they may be a “defect” due to a “pathological situation” that ultimately causes “chronic inflammation.” In other words, the design that Lents demands must exist does in fact exist in a significant number of people — but Lents’s version of a good design may actually not work very well. To see why this is the case, you need to understand why a basic premise of his arguments — that our sinuses drain primarily due to gravity flow — is mistaken.
Egnor Was Right Again
Lents’s main argument is that most of our sinuses use gravity drainage, but since the ostium (opening) of the maxillary sinus is found at the top of the sinus, this represents “poor design.”
Egnor noted that the paranasal sinuses “don’t drain primarily by ‘gravity,’ as Lents naïvely asserts.” Again, Egnor is right and Lents was wrong. While gravity drainage is used, to some extent, by all of our paranasal sinuses, it is not the preferred drainage mechanism of any of our paranasal sinuses, and the mechanism of drainage of the maxillary sinus is no different from any of the other paranasal sinuses.
Isn’t this counterintuitive? Not if you think about it. As explained by the famous ear-nose-throat surgeon Sidney Yankauer in a paper, “The drainage mechanism of the normal accessory sinuses,” the openings of the paranasal sinuses are all located in different orientations. That way, “there is no single position of the head which is favorable to drainage from all the sinuses.” He further notes that even when the head is in a favorable position for gravity drainage of a particular sinus, gravity drainage would “at best, be only slow and intermittent.” That is because sinus drainage tubes are small and narrow, and the mucus thick and viscous. Thus, “if the liquid is thick and viscid … like the nasal secretions, its escape will be very slow; in fact, if the opening is very small, there may be no escape of liquid at all.” Moreover, he observes that when a liquid is present in small quantities, as is the case with mucus, “the adhesion of the liquid will overcome its gravity” and it may not flow downward.
Yankauer observes that our sinuses normally have no trouble draining themselves:
The fact that the sinuses are thus capable of draining themselves when they are in a normal, healthy condition will hardly be disputed; but that they are also capable of emptying themselves through their natural orifices when they have become diseased may not be so self-evident. Yet it is within our experience that acute inflammations of all the accessory sinuses have a natural tendency to get well without operative interference, the end of the disease being marked by a discharge of secretion into the nose, lasting for days or weeks, during which lime drainage through the natural orifices goes on without interruption; so that even when the mucous membrane is diseased and the quality of the secretion altered, drainage through the natural orifices is possible, and in a large percentage of the cases is sufficient.
How do we reconcile these observations — that there is no single position of our head that is conducive to gravity drainage of the sinuses and that gravity drip of our viscous mucus through the narrow sinus passages would be very slow, and perhaps even prohibited by liquid adhesion, yet our sinuses normally seem to have no trouble draining? This is because, as he observes, gravity is not the primary mechanism of drainage of our sinuses:
Considering these facts, and bearing in mind that the secretion of the healthy sinuses is a mucous fluid, and that of the diseased sinuses a still more viscid one, it is evident that gravitation, as such, plays a very small part in the drainage of the normal accessory sinuses.
This is exactly correct. For example, consider our frontal sinus (see the image above for its location). Lents claims in his book that the frontal sinus (directly above the narrow between the eyes) “can drain downward.” This is true, but his implication is that frontal sinus drainage is primarily due to gravity. That is inaccurate.
The frontal sinus does ultimately drain downward, but not primarily due to gravity. It drains only after cilia sweep the mucus in a circuit which first goes upward, and then comes back around down the other side of the sinus in a circle, thus draining downward. This is seen in the frontal sinuses depicted in the diagram below:

In the diagram, roughly redrawn from slide 35 of this lecture, and a diagram at this medical anatomy library, you see that the drainage ostium is at the bottom (near point A), right where Lents says it should be. But with mucus starting at point A in the frontal sinus, the mucus does not always drain directly downwards. Instead, on one side of the ostium, mucus travels along a circuit (shown by the turquoise arrows), first upwards (against the force of gravity) along the interior of the sinus, around the top, and then finally draining along the bottom of the sinus and then out.
A Circuitous Route — For a Purpose
Why would mucus in the frontal sinus take this circuitous route? The answer is simple, from a design perspective: Mucus has an important purpose and, as the Yankauer observes, gravity drainage is not an efficient mechanism even when the drainage port is located at the bottom. With only gravity at work the frontal sinus would dry out and mucus would fail to cover the entire sinus and do its job of sweeping away bacteria and other harmful foreign bodies. The roundabout route ensures that mucus is swept across the entire sinus, keeping it moist and allowing it to do its job.
The key point is that the main mechanism of sinus drainage — even when there’s a drainage port at the bottom as in the frontal sinuses — is the cilia, not gravity. Yankauer writes:
the explanation of the manner in which these cavities are drained, must be sought in a study of the character of the mucous membrane over which this drainage takes place, and of the physical properties of the secretion. With the exception of the olfactory tract proper, the mucous membrane of the nose and its accessory cavities is covered with ciliated epithelium. The cilia are in a state of constant motion, which has been compared to the lashing of a whip. Each cilium moves through an arc of from 20 to 30 degrees, at the rate of about 12 times per second, the forward movement being about twice as rapid as the return movement. All the cilia of a single cell move in the same direction at the same time, but the cilia of all the cells do not move simultaneously, but the motion is carried over the mucous membrane in a wavelike manner. … The power exerted by the combined action of the cilia is said to be very considerable.
Consider this passage from a much more recent article, “Paranasal Sinus Anatomy and Function”:
Since many of the sinuses develop in an outward and inferiorly fashion, the ciliated mucosa often moves material against gravity to the sinus’ exit. This means that mucus produced just adjacent to a sinus ostia, if it is on the afferent side, will travel around the entire sinus cavity, often against gravity, before exiting the ostia. This is one reason that creation of accessory ostia at sites outside the physiologic ostium will not significantly improve sinus drainage. In fact, this sometimes results in mucus draining from the natural ostia reentering the sinus via the newly created opening and cycling through the sinus again.
What Did We Just Read?
First, “mucus produced just adjacent to a sinus ostia, if it is on the afferent side, will travel around the entire sinus cavity, often against gravity, before exiting the ostia.” This shows that gravity drainage is not necessarily the preferred mechanism of sinus drainage even when the drainage hole is on the bottom and mucus is produced right next to the hole.
When a sinus has the “good design” that Lents claims it should have, it actually drains more like the sinus that he claims has a “poor design,” moving mucus upward via cilia against the force of gravity.
Second, we see that, because gravity drainage is not the preferred mechanism of drainage, creating new holes in the sinuses where you think gravity would help improve the drainage might not be a good idea. That would interfere with the natural circuits of mucus flow as driven by the cilia. This is consistent with the aforementioned observations of problems associated with accessory ostia in the maxillary sinus. When the design that Lents demands exists is actually implemented, it doesn’t work very well.
Lents in his book acknowledges that cilia move mucus around. But the question for him is this: If it’s so important to have drainage ports at the bottom of a sinus, then why is it in the frontal sinus that much mucus that starts off right next to the drainage port at the bottom is swept upwards away from the drainage ostium by the cilia and around the entire sinus before it flows out of the ostium, completing a full circuit? The answer is that gravity drainage is not very important to sinus drainage. The premise behind Lents’s argument for poor design of the maxillary sinus is false.
There’s another reason that ciliary movement is preferred: People don’t spend all their time standing upright, so gravity isn’t always tugging on our mucus in the same direction. In fact, we spend about a third of our lives sleeping, putting our head in positions that would not work well for spreading mucus around the sinuses if gravity were the main force. Thankfully, it isn’t, and we have cilia wisely designed to move the mucus where it needs to go.
That’s not to say gravity drainage plays no role. There may be another good reason for the presence of the ostia at the top of the maxillary sinuses — one that Nathan Lents writes about, but that he misidentifies as a design flaw. Lents writes:
The poor location of the drainpipes in the maxillary sinuses also helps to explain why some people with colds and sinus infections can briefly find relief by lying down. (p. 11)
Maybe that’s another key to understanding the design of the maxillary sinus and the location of its ostium: its opening at the top is designed to give relief when a person is sleeping, so that he can sleep.
Asking the Right Questions
This is all an admittedly lengthy way of saying that Lents has identified no design flaw.
Does that mean all the questions raised by nasal physiology are answered? Hardly. But Egnor’s ID perspective led him to ask important questions about the design of the sinuses:
Lents ironically makes a point that design scientists have been making all along: consideration of design principles leads us to a much deeper understanding of biology. Is the maxillary ostium an overflow drain? Why does drainage normally move uphill by ciliary action, rather than downhill by gravity? Why is there only one ostium in the maxillary sinus, rather than many? To what extent does the drainage of mucous depend on flux of the water component of the colloid back through the mucosa, rather than through the ostium? These are all good questions, and they are the kind of questions that lead scientists to a deeper understanding of physiology. They are, of course, design questions.
These are exactly the right questions, and investigating them from a design perspective has helped us to understand why ciliary motion rather than gravity is the preferred mechanism for moving mucus around the sinuses.
Photo credit (top): StewartENT, via Pixabay.